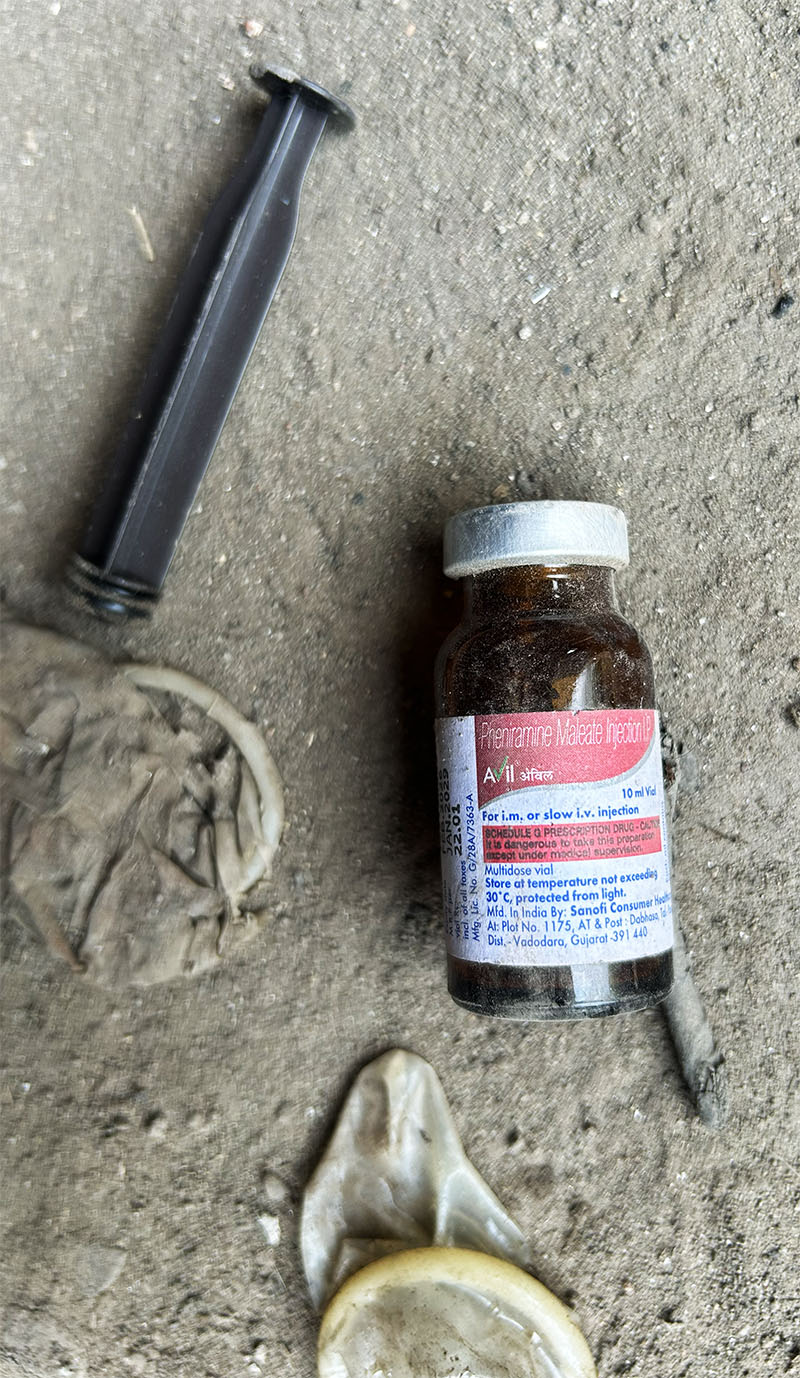
HIV spreads along Nepal-India trucking routes where long-haul drivers and transgender sex workers intersect and where treatment gaps and social stigma make both groups especially hard to reach.
He learned about HIV the way many drivers of his generation did: by watching a friend die of it. He has driven in 26 Indian states and union territories, from Jammu and Kashmir to Kanyakumari. He has driven trucks, tourist buses and Maruti cars fresh from factories. For two years, he drove a bus at the Delhi airport. He has taken pilgrims from Nepal to Odisha and back. Once behind the wheel, he could go 24 hours without stopping. “Buses are easier,” he said. “Passengers are not that heavy. Trucks carry a lot of heavy loads.”

He is 46 years old and HIV-positive. He gets his medicine from Janakpur Provincial Hospital in Nepal’s Terai region.
“I had a friend from Rajasthan who also drove company vehicles,” he said. “He became very sick. Nothing seemed to help him. He had constant headaches and stomach pain. There was another friend named Banwari who suggested taking him to the hospital. When his blood was tested there, they said it was HIV. At that time, there was no HIV medicine. The doctor called his relatives, gave him an injection and asked them to take him home. After reaching home, he died within one and a half hours. That is how I learned about it.”
He does not evade the question of how he contracted the virus. “I am a driver, I will speak openly,” he said. “I was not at home much, only coming back once every six to seven months. At that time, there were places every kilometer. Along the highways, on both sides, in Bombay, Pune, Malegaon, Dhule and Nashik, all those places in Maharashtra. Also, in Rajasthan like Kotputli, Sikar, Jaipur, Kishangarh and the Nathdwara bypass. Friends used to say, ‘Let’s go there.’ We used to go together in groups of five to seven trucks from different companies.”
He found out about 17 years ago, when his eldest daughter, who was frequently sick from birth, was finally tested at Darbhanga Hospital and tested positive. He and his wife went to a health post at Safi Chowk in Dhanusha the same day. Both tested positive. His first wife died. They took her to Dharan and kept her in the hospital for 15 days but she never came home. His eldest daughter, who was 25, has also died. Two of his brothers have died. He now raises their children alongside his own.
His second wife left him after she learned about his HIV status. She now lives at her maternal home in Dhanushadham. Their relationship deteriorated after the diagnosis and she has been away for two years. He does not say much about this.
“In my truck line, nobody knows about me,” he said. “When driving, if others see, they ask, ‘What medicine is he taking?’ They don’t understand my situation.” He hides his pills. He cannot go far from Janakpur. He cannot go abroad. “If I were healthy,” he said, “I would have gone abroad and earned money. I earn here too, but only enough to survive.”
He drives taxis now, mostly on night shifts, along the Hulaki Highway between Janakpur, Siraha, Rajbiraj and Biratnagar, often spending up to 15 hours on the road. Whenever he gets the chance, he still takes long-distance tipper truck work, sometimes for 12 or 13 hours, and occasionally 24 hours straight.
India and Nepal share a 1,751-kilometer-long border across five Indian states: Sikkim, West Bengal, Bihar, Uttar Pradesh and Uttarakhand. About 700,000 Indians live in Nepal, while reports estimate between 1 million and 3 million Nepalis live in India. India’s response to HIV among long-distance truck drivers is, by the government’s own account, a public health success story.
Since 1992, through four phases of the National AIDS Control Programme, the government cycled through successive rounds of targeted intervention backed by World Bank credits totaling $807 million. The logic was epidemiological. Studies showed that 36% of truckers across India were clients of commercial sex networks, including female sex workers, transgender sex workers and men who have sex with men, making them what public health workers call a bridge population between core high-risk groups and the general public.
Around 2057 BS (2000), another Nepali driver had a serious accident in Punjab. His right leg was fractured and a rod was inserted. He drove on it until the rod broke internally. He was taken to Patiala Medical College, a government hospital, where he was kept for 15 days, remaining unconscious for three of them, and given multiple blood transfusions. The government hospital said nothing about HIV. Two months later, when the rod failed, he went to a private hospital, and they told him.
“I didn’t believe it,” he said, “Because until two months earlier, my treatment was still going on and they had not told me anything. Because of that, I got married three to four years later.” He married in 2061 BS (2004). He has a son and a daughter, neither of whom has been tested. His wife lives separately. “We have been living separately for four to five years. Maybe she has it too but maybe it hasn’t affected her.” He hasn’t told her.
He now drives taxis rather than lorries. His vehicle runs from Delhi or Punjab directly back to Nepal. Every three months, he travels to the ART center in Butwal to collect his medicine, a round trip that, factoring in his work, takes roughly two and a half months to complete. The ART center calls him two weeks ahead of his pickup, using phone calls or WhatsApp if the call doesn’t connect.
On a long taxi run, he can go 24, 30 or sometimes 36 hours continuously. In that stretch, timing shifts. “Sometimes I miss them when I’m busy working. One or two days in a month may be missed. But my reports are fine.”
He does not feel the need to tell anyone. “It’s a personal matter,” he said. “So, it doesn’t feel right to tell others. I am happy with my life.”
In Delhi, a driver who left the trucking line 11 months ago found out while getting a hernia checked in his home village in Vaishali, Bihar. “I was having a fever and was taking a lot of medicines but it wasn’t going away.” The test he took for something else flagged something entirely different. “I came out HIV positive.” He had known about the Apollo Tyres Foundation clinic at Sanjay Gandhi Transport Nagar, Asia’s largest trucking hub in northwest Delhi, where 40,000 trucks move in and out of the capital daily, from his years in the business. He came in, asked to be tested, and the result came back positive. The formal outreach hadn’t found him. The disease found him first, on its way to something else.
He no longer drives. Every morning at 6, he pushes a juice cart to the pavement outside a local hospital and sets up for the day, catching the early foot traffic. He earns around 7,000 rupees a month, half of what he used to make as a truck driver. His children study in a government school. His family knows. The initial fear, he says, has passed. “Now there is not much fear. As long as the medicine goes on, I will live.”
Transport Nagar, Delhi. Yash Sadhak Shrivastava/NIMJN
He takes his antiretrovirals before anything else each morning. “On any day, I will take the medicine, only then will I go to any work. Medicine is important.”
He is also clear about the disease’s arithmetic. “It is not necessary that if we do a wrong deed, only then will the disease happen. An infection can also spread to a good person. The one who doesn’t do this deed, it spreads to them too. The one who does it, theirs spreads quickly. This thing doesn’t happen instantly. If someone violates something today, it shows after four to five years.”
Three men. Three diagnoses that arrived years late, through a daughter’s blood test, an accident in Punjab, a hernia checkup. None of them knew they were positive while they were still on the road.
“HIV prevalence appears to be higher among those who are either illiterate or are only primary literate. HIV prevalence was highest at 0.59% among those who reported having a spouse occupation as truck driver/helper,” according to a report published by the Ministry of Health and Family Welfare, Government of India.
The people positioned closest to drivers on this corridor, the ones who have the conversation about condoms before a doctor ever gets the chance, are the transgender sex workers and outreach workers who work the transport nagars, dhabas and night streets of India and Nepal.
THE HUB
Sanjay Gandhi Transport Nagar at dusk looks nothing like a neighborhood and everything like a staging ground. Long rows of heavy vehicles line the internal roads and open parking lots of what is Asia’s largest trucking hub. The lighting is functional and uneven, streetlamps, truck headlights, workshops and roadside dhabas all contributing their own pools of light against the dark. In abandoned multi-story buildings near the inner roads, doors hang open on broken hinges. These buildings have been vacant for years. After dark, this is where some of the night’s transactions take place.
Bala Devi has run her dhaba here for 30 years. She is 60 years old, wears a simple saree and a pair of spectacles, and carries herself with quiet confidence. From behind her counter, she greets drivers with the ease of someone who has spent three decades in the same space, working from nine in the morning until midnight alongside her son, who is around 30. On the wall behind her hangs a banner listing available medical services: testing, check-ups, referrals. Drivers look at it and ask her what it means. They tell her son about symptoms, sores and discharge because they are embarrassed to tell her directly. She overhears. She sends them to the clinic.
She has been connected to the Apollo Tyres Foundation since 2002, when the foundation staff began organizing street plays near her dhaba and put up their banner. “Some truck drivers would ask me what the program was about. I would tell them that Apollo Tyres had a clinic for truck drivers where a doctor was available and medicines were provided.” Her first clear memory is of a driver who came in with discharge and sores. She sent him to the clinic. He was back in a few days and recovered. Her son handles what she can’t. “He also attends Apollo Tyres Foundation meetings and is directly connected with the clinic. Why would he need to ask me? He takes them there himself.”
At night, when the kitchen closes, 10 to 12 sex workers come. They know Bala Devi. They buy jute sacks from a shop nearby, 10 rupees each, fold them under their arms, and head for the abandoned buildings or the space under the trucks. There is no hierarchy among them. They come from different areas. “I tell them, ‘You can go anywhere but don’t come to my hotel,’” Bala Devi says. “Still, if they come, I tell them, ‘Whatever you need, condoms or anything else, you can take it from me.’”
The Apollo Tyres Foundation clinic is not visible from where they work at night. But the Apollo Tyres banners can be seen from those abandoned buildings. The distance between the banner and the service it advertises is one of this story’s recurring measurements.
Mayra Mehraf has worked as an HIV outreach worker at the transport nagar for a year and a half. Before that, she spent three years doing HIV work in the transgender community. She describes what dusk looks like at the hub. “After six, as it starts getting dark, female sex workers come here to the truck driver brothers. Now that I have come and I am from that community itself, a thought goes around that perhaps if I approach, will this also happen? So, this has happened to me many times.”
She reaches drivers by starting somewhere other than the disease. “I make liaison with people, talk to the driver: okay, from where have you come? There mangoes are very famous, these things are that. So, they engage a little.” The HIV conversation opens only once the driver is present with her. Drivers who refuse condoms tell her: “Those who come from specific states, they say directly that they don’t get any pleasure from condoms. ‘After doing this, there is no feeling at all, so how can I have intercourse with you?’”
She has also encountered a population at the transport nagar that no program formally reaches: trans women from Bangladesh, Guwahati and Assam, making 20 to 25 encounters a night. She asked how they managed. “They told me they take medicines, some green leaf tablets. They didn’t even know the name of the tablet.”
The economics she describes are structural. A transgender sex worker working in a particular area pays a percentage of her earnings to a Guru, the senior community member whose territory she is in. The percentage is fixed. So, when a night goes badly, the calculation is simple: fewer clients at higher prices, or more clients at lower ones. “Those who are not beautiful, so for them, what happens is they have to do it even for Rs 200,” Mayra says. “So, for them, what happens is they increase the clients then. ‘I have to earn this much, this much I have to give to the Guru, this much I have to keep for myself.’”
THE WORKERS
A UNAIDS report found that in 2022, the relative risk of acquiring HIV was 20 times higher for transgender women than for the wider adult population globally, up from 11 times higher in 2010. In India, data from NACP’s programmatic mapping shows that while the overall adult HIV prevalence stands at 0.20%, the figure among hijra and transgender persons reaches 3.78%. The range across all key populations runs from 1.85% among female sex workers to 9.03% among people who inject drugs.
Highway-based sex workers in Nepal, tracked through Integrated Biological and Behavioral Surveillance surveys, showed HIV prevalence declining between 2004 and 2016 but stabilizing at around 2% to 3% in some areas, a population that researchers continue to identify as high-risk due to mobility, cross-border movement, contact with truckers, and inconsistent condom use. In Nepal, of the 27,054 people currently on antiretroviral therapy, 510 are recorded as transgender, a figure that officials acknowledge is almost certainly an undercount, given how many hide their status.
“Laws that criminalize transgender people drive people away from the support and services that can help them protect their health,” the UNAIDS report noted. “Often, transgender people experience multiple intersecting forms of discrimination. Transgender people are disproportionately more likely to enter into sex work.”
An HIV-positive transgender sex worker who works along the highway bypass in Delhi found out she was positive 9 years ago through an NGO. “The ground slipped from under my feet. I used to take medicines secretly at night at home, so my family members saw: ‘What are you eating like this?’ So, I said I am taking medicine to get fat. Then later they came to know about it. Then I left my home. Since then, I have lived with transgender people separately.”
She also counsels alongside sex work, talking to every new driver. “Every time a new driver comes. From different areas, a new driver comes. I ask, where have you come from? Because it’s their need, they need it because they are sitting in a hot seat. They also tell us this, that we are very hot, so we have to release our heat.” She gives condoms to drivers who don’t have them and extras after. She tells each one, “Don’t do it without a condom. It’s not written on anyone’s face whether they are HIV positive or not.”
She also describes what she hears when a drunk driver talks. “The truck driver comes. ‘Oh, come on, I had done it with her, I had gone to Punjab, she gets it done without a condom, man, it gives so much fun. You also get it done.’ So, then I understand that he must have done it with who knows how many.” On drivers who know they are positive and say nothing, “Some truck drivers don’t tell that they are HIV positive. Even if they know, they still won’t say.” She won’t take extra money for unprotected sex. “I know about myself that I am HIV positive, so will I do something like this to others? Rather, I would want the other person not to go through my situation.”
The former truck driver from Delhi is careful about how he explains what happens on the road. “When the family is far away, people live like that. On long routes, these are the problems. Fatigue remains. To feel happy, a person needs something else. No matter how good a thing you feed them, they are not satisfied.”
Another transgender sex worker described what happens at Azadpur Mandi in Delhi. When one driver insisted on sex without a condom, a colleague found a way around the refusal. “She was a very clever hijra. She put a condom in her mouth and put the condom over his penis. He didn’t even realize it and she also took the money. Knowledge itself is a protection.”
The road runs on substances, too. A 2020 survey by the SaveLIFE Foundation of 1,217 truck drivers across 10 Indian cities found that 36% admitted to sometimes driving under the influence of alcohol or drugs, and about 5% said they always did long working hours and the need to stay awake being the most cited reasons. “Without drugs, no person, driver or conductor exists,” the Azadpur sex worker said. “Those who travel long distances will drink for sure. Whether they use bhang, ganja, smack or alcohol, some form of intoxication is necessary for them. Otherwise, their bodies cannot handle such a long journey.”
In Kathmandu, a transgender sex worker acquired HIV during her very first sexual contact, a man she met on Facebook. She was 17. She is 26 now.
She had been identifying as a man at the time and could not bring herself to speak openly with doctors about what had happened. For more than two months, she visited a hospital in Palpa with symptoms that would not resolve. The doctor gave her treatment but never indicated HIV. She reached out over social media to Babu Dumi Rai, a non-binary trans activist working in the sexual health sector in Bagmati Province, who arranged for her to be tested in Kathmandu. The result came back positive. She later found out that the man she had met on Facebook had already known his status.
“After some time, I became ill. I kept going to hospitals but the hospital did not directly test for it. When I got tested elsewhere, I was found HIV positive. After that, I felt like I was going to die.” Following her diagnosis, she was invited to a USAID program where she and others received confidential counselling, the beginning of her own outreach work. She now counsels on the street alongside her work. “Drivers still lack awareness. They need education classes about sex, diseases, HIV and STIs. Many people do not even know about STIs apart from HIV. Especially, people from the Terai region do not want to use condoms. I feel HIV is more prevalent in the Terai than in the hills.” Some clients secretly remove condoms during intercourse. “At night, it is even more difficult.” She tells clients who offer extra money, “The pleasure of a few minutes should not ruin your entire life.”
She watches what has been lost since the international funding cuts. “Earlier, there were clinics where STI and HIV testing were done, but now people do not come for checkups. Earlier, people used to come even hesitantly because it was our office and it was from our own community. Now, when people go to private or government hospitals, they are not accepted properly. In many places, they are looked at with negative judgment. Once they hear ‘trans’, they are treated as if they are from another planet. Now, after the project has ended, it feels like HIV is spreading more.”
Babu Dumi Rai hears from sex workers about what clients expect. “Being away from their families and partners, they too feel the desire to be sexually active. When it comes to whom they engage with, they often go to street-based sex workers. And after finally paying money, there is a mentality of asking, ‘Why should I use a condom after paying?’”
She describes what happens in hospitals. “Even in hospitals, people ask, ‘What is your gender?’ From every counter all the way to the counselling room upstairs, there is a process where we are forced to justify ourselves repeatedly. Because that process is so troublesome, our third-gender community is also not seeking medical treatment. That, in turn, affects not only us but other communities as well.”
THE BORDER
Dr. Nikesh Shah works in the ART outpatient department at Sukraraj Tropical & Infectious Disease Hospital in Kathmandu, which has registered more than 6,000 patients since it began ART services, with around 2,500 currently active.
He explains what missing even a day means. “HIV is not a virus that completely disappears from the body. It hides somewhere. The medication prevents the virus from replicating. If medication is missed for one or two days, viral replication increases again. The virus starts multiplying.”
The cascade from there: the first-line drug starts to fail. “In Nepal, India and many Asian countries, ART options are limited. If one drug fails, we move to another option. If that also fails, we may not have a third option.”
According to a fact sheet published by the government of Nepal, over 34,000 people are living with HIV.
Radheshyam Shrestha, Program Coordinator at AHF Nepal, describes the pattern that emerges at Sukraraj. Around 10 to 12 patients stop treatment every month. The hospital calls before appointments and checks whether the medicine stock is running low. “Even after doing all this, some clients still get lost.” When AHF investigated, the answer kept coming back the same way: patients had gone to India for work and could not access medication there.
The reason is administrative. At Indian ART centers, drivers are asked to produce a ration card, an Aadhaar, or a voter card as proof of address, which Nepali nationals do not carry. They are also asked how and why they acquired HIV. Many leave without medicine. Some contact ART centers in Nepal by phone, requesting supplies to be sent through NGO intermediaries. AHF Nepal has recently arranged a direct visit by representatives from the Nepalgunj ART center to the Lucknow ART center to discuss easier access.
Kranti Kumar, a staff member with the National AIDS Control Organization (NACO) at Maharajganj District Hospital in Uttar Pradesh, said the nearest Community Health Centre (CHC) to the Sunauli border is in Laxmipur block, around 30 km away, while the Maharajganj District Hospital is about 60 km from the border. Both facilities provide HIV testing and antiretroviral therapy (ART), he said.
India’s National Operational Guidelines state that treatment should not be denied to patients who cannot produce valid identity documents. NACO did not respond to requests for comment.
The mechanism designed to address this, a government-to-government agreement between Nepal and India, does not exist for HIV. Dr. Samir Kumar Adhikari, Deputy Spokesperson for Nepal’s Ministry of Health and Population, confirmed that while formal cooperation exists for malaria and other diseases, there is no official agreement with any Indian agency specifically on HIV. Dr. Man Bahadur K.C., Chief Medical Officer at NCASC, acknowledged an informal understanding in practice but said his office has not formally received complaints about Nepali patients being denied ART in India. “We need to first investigate, through our 96 ART centers in Nepal, the exact reasons why some individuals are unable to access medicines in India. If necessary, we can then seek further support from India. So far, we have not received such complaints.” Dr. Adhikari said, “Until now, this issue has not been included in the G2G framework. If problems arise and complaints increase, we will discuss them with the relevant stakeholders and work on them accordingly.”
Sushil Khatri, chairperson of SPARSHA Nepal, names the mechanism that was supposed to fix this. “There was once a G2G coordination between Nepal and India, but it later became weak. If someone from Nepalgunj goes to work in Lucknow, the ART center in Lucknow does not provide medicine because a ration card is required, which Nepal does not have.” AHF Nepal tries to bridge the gap by sending patients heading to India up to six months of medicine, with NGOs providing formal guarantees. But this requires the driver to disclose his status before he leaves, something most won’t do. “There is a high risk that if their HIV status is disclosed, they may lose their job,” Shrestha said. “Because of this fear, instead of staying connected with us, they prefer to stay without taking medicines.”
Health information centers have been established at the Gauriphanta border point in Dhangadhi and at Sunauli, where testing and counselling services are available. But there is no budget to expand further and no ART center exists at the border on either side.
Sandeep Jain, president of the Traders Welfare Association at Sanjay Gandhi Transport Nagar, Delhi, who has run his transport company from the hub for 30 years, identifies the chokepoint precisely. “The truck that runs from Delhi to Nepal reaches the Sunauli border on the third day. When they reach the Sunauli border, their truck faces a break of two to three days there. That two-to-three-day stopping point seems the most problematic to me.”
A few months ago, an NGO came to Jain to enquire about a driver who had tested positive but had stopped engaging with services. “We called the driver, too, but the driver never returned to that NGO.”
The Nepali driver who drove to 26 states has watched what happens when men cannot or will not manage their treatment. A man he knows in India carries medicine from Nepal but sometimes misses doses for two or three months. “Doctors scolded him. They told him, ‘If you cannot manage medicine, why go outside? Stay in Nepal.’ But he ignored it. He is still weak.” Two people in his own village refused treatment entirely. “I advised them to take medicine but they refused, saying they were fine. They died within two months.”
Dr. Shah at Sukraraj identifies stigma as the single largest reason patients disappear from the register.

“Many people still hear the word ‘HIV’ and immediately think it is something bad. There is a belief that it is a fatal disease. Because of this, if someone is HIV-positive, they try to hide their status so that others do not find out. They isolate themselves, avoid treatment, stop taking medication, or do not come for follow-ups.” Khatri describes the specific form it takes among drivers: “Even if they are taking medicines like sleeping pills, gastritis medicines, or vitamins, they fear disclosing that it is HIV medicine. Because of that fear, they hide it.”
The Delhi driver explains his own calculus. “They fear that the family might find out that he does wrong deeds, this and that. Reputation, this is what they think. That’s why people don’t want to bring the matter forward.” He himself has moved past it. “If we had hidden this matter, it would have been our loss, right? The disease is inside our body, and if we sit hiding it, what will we get? Our own life is ruined.”
The Nepali driver who got the blood transfusion in Punjab, who drives taxis now, who has not told his wife, and who misses a day here and there, has not moved past it. “It’s a personal matter. It doesn’t feel right to tell others.”
THE GAP
The numbers tell one story. HIV prevalence in India has declined from 0.33% in 2010 to 0.20% in 2024. Annual new HIV infections nationally have fallen from 1.25 lakh to 64,500, a 49% reduction. AIDS-related deaths are down 81.4%. In Nepal, new infections fell from 5,545 in the year 2000 to 614 in 2024. The people who helped in that reduction are leaving the industry.
Jain estimates that 60% of India’s truck drivers today have joined the workforce in the last 15 years. A driver begins at around 20 or 22; by 40, he has retired, bought his own truck, or moved to other work. The older drivers, the ones who sat through the awareness sessions, who watched colleagues die, who understood viscerally what the disease could do, have gone home. Their children are now driving. “That new generation also needs awareness,” Jain said. “The older ones have gone home and they don’t talk to their children about HIV after going home. The environment is not that open yet.”
In Nepal, a National Demographic and Health Survey found that only 15% to 20% of young people said they had knowledge about HIV. Shrestha at AHF Nepal frames the gap plainly, “That means we still need to increase awareness about prevention. Otherwise, there is a chance it may increase again. Earlier, around 2004, prevention was also widely discussed. Awareness materials were produced. But now that is not happening.”
A World Bank report on India’s NACP found that behavior change communication remained a consistent weakness. “Most key informants thought the behavior change communication component is a weakness.” Social media campaigns failed to reach high-risk groups and ‘mainly reached the general population’. Stigma reduction efforts using mass and mid-media were judged to ‘only look good on the surface’.
Amit Ranjan Chaudhary, who has managed the Apollo Tyres Foundation programme for 15 years, confirms this from the field. “Whenever our visits happen at other locations, we see that if we talk to any new driver, they don’t have much information about our services or about HIV. We have been working for the last 25 years, yet we find such people who do not have any information.”

In Fiscal Year 2025, Apollo’s program had more than 1,100 peer volunteers across 35 locations, 87 female and 102 transgender, periodically replaced as individuals leave. Bala Devi, at 60, is still behind her counter. Her son, who is 30, takes drivers to the clinic without being asked. Someone will have to do the same in the generation after them.
NACP Phase V (2021–2026) is the first phase fully funded by the Government of India, at Rs. 15,471 crores, approximately $1.6 billion, over five years. In January 2025, the United States froze all foreign assistance, including PEPFAR. The impact on India, where the government had already absorbed much of the program, was less acute than in high-dependency countries.
But in Fiscal Year 2024, the US had disbursed approximately $17.74 million for HIV/AIDS programs in the country, supporting HIV testing, treatment, laboratory strengthening and technical assistance to NACO through a range of NGOs and university partners, including Johns Hopkins University, PATH, Voluntary Health Services (India), SHARE India, the University of Washington, Sattva Consulting and others. That ecosystem has not been protected. Across Telangana, around 33 clinics that once catered specifically to people living with HIV have been struggling to function since the funding cut. Many NGOs and drop-in centers are operating with skeletal staff or have shut down entirely.
Apollo Tyres Foundation had already moved away from international funding. Its last FCRA grant came in 2017, for the first year of a project; no comparable funding has come since. “What we actually looked at was more from the point of view of how we can involve the community, organizations, corporates and the government,” said Rinika Grover, who heads Sustainability and CSR at Apollo Tyres Limited.
In Nepal, the situation is more precarious. The government allocates only around 5 to 7%% of its total donor budget to HIV programs, and the health budget has been shrinking year by year. Under Global Fund Grant Cycle 7 (2024–2027), Nepal received a total of $44 million but only around $600,000 was allocated to the HIV department. For the next cycle, Global Fund support is projected at a similar level but allocations are unclear and officials expect the HIV share could fall further. Active donors include the Global Fund, the US Embassy through direct funding, UNDP, and AHF Nepal.
“Each year, only around 5 to 7% of the total donor budget is allocated to HIV programs under the government department. However, in the coming years, we hope the government will allocate at least 10 for HIV programs,” said Dr. Sarbesh Sharma, Director at Nepal’s National Centre for AIDS and STD Control.
“Today, the Government of Nepal itself purchases 100% of ART medicines,” said Khatri. “Around 25,000 people are on treatment. There is no shortage of medicine. But prevention work is not strong enough. Treatment is available after infection and prevention is still weak. We are still in a concentrated epidemic stage.”
Dr. Sarbesh Sharma acknowledged the asymmetry. “The treatment is expensive, and the government bears the direct cost. But this does not mean we are not working on prevention. We have done as much as we can but it is still insufficient. Many people are still not tested. Some may be hiding their status due to stigma and others are lost to follow-up in the system.” He added, “It is not possible for the state to eliminate HIV at once. The work has to continue and we also have to consider the country’s limited resources.”
Near the end of a conversation, almost as an afterthought, the former truck driver from Delhi said, “Like how earlier companies had made people aware, after 10 years, five years, they will have to make them aware again, right?” He said it without accusation or urgency, as though it is the most obvious thing in the world. As though it should already be happening.
RUNNING OUT
Running underneath all of this, the outreach, the medicine, the stigma, the generational gap, is a condom shortage that has been quietly building in Nepal and India, and threatens to deepen across the region.
Dr. V. Sam Prasad, Country Program Director for AHF India Cares, flags the supply chain risk. “There is news coming out that condoms in India might also get affected because the ammonia and silicone, which are imported from other countries, might be stuck because of the war in the Middle East. We might face some kind of backlog in the production as well as distribution of condoms in the future.” A disruption in the global supply chain reaching into the truck stops and dhabas of India, through a chain of causality that runs from a war in the Middle East to a used condom in the dirt at Sanjay Gandhi Transport Nagar
Babu Dumi Rai is specific about where the responsibility lies. “Rather than saying it is because of the war, it sometimes feels more like an excuse by the Government of Nepal because the government usually imports condoms every year through advance booking. This explanation about war has been given for some time but the shortage had already existed for around one and a half years.”
The government confirms the gap. “Condoms have been in short supply for a long time,” said Dr. Sharma. “The Government of Nepal procures them only for the Safe Motherhood program. We have never procured them specifically for HIV prevention. When donor funding was available, we used to send funds to district health offices to purchase them. But now, even that funding has stopped coming.”
Khatri explains the structural reason, “Condoms are only seen as a family planning tool. They are not viewed from the perspective of HIV, hepatitis and STI prevention. Because of that, procurement is not designed for disease prevention.” The government counts expected pregnancies when ordering condoms, not expected exposures to infection.
Babu Dumi Rai says what she thinks this means. “I feel that next year, HIV infections are going to increase. People may say our community is small but as it spreads peer to peer, it continues expanding.”
Ashok Khurana, a Delhi transporter who has been in the business since 1978, remembers a stopping point called Mandla in Madhya Pradesh on his old Delhi-Raipur route. “There was so much of this sex work that there was no vehicle that wouldn’t stop at Mandla.” He remembers Bombay in 1986, a place drivers called Dimland. “There was a whole hub of sex workers there. Many drivers fell victim to AIDS from there.” He says the situation is much better now. “I haven’t seen any driver with HIV anymore. They sit right next to me but the disease isn’t there now. India has improved a lot. Otherwise, there was a time you’d hear every day: ‘That driver is infected, he’s lying sick there, he’s dying there.’ They wouldn’t tell anyone until the end and then we’d find out, ‘Sir, he passed away.’”
The drivers Khurana remembers are mostly gone. Their children are on the road now.
The Nepali driver who drove to 26 states and UTs has heard about a long-acting injectable form of ART being developed. One dose every six months, no daily timing, no race back to a dispensary, no pills to hide from colleagues who would not understand. “They say injections will come for six months or a year,” he said. “But who knows when?”
He asks without bitterness. It is a practical question from a practical man: when does the medicine learn to travel as far as the work does?
The former Delhi driver who pushes his juice cart out each morning has already answered it in the only way available to him. “There should be medicines available on the highway,” he said. “There will be less trouble for drivers this way or else in a different country, how do we know about the availability of a hospital?"
He takes his medicine before he does anything else in the morning. He has made that the first rule of his day. What he is asking is whether the system is willing to make the same commitment he has, to treat the disease as the first item on the agenda, not an afterthought to family planning targets and bilateral paperwork.
___ ___
Interviews were conducted in Hindi and Nepali and translated for publication. Names of transgender sex workers and truck drivers have been withheld.
Please adhere to our republishing policy if you'd like to republish this story. You can find the guidelines here





Comments